DISCLAIMER: The article which this post is reporting on looked at policies related to alcohol and substance use only through 2016. Since 2016, some states have updated/changed their policies, which is not reflected in the article or this post. For example, North Carolina does, in fact, have a policy related to priority access to treatment. A follow up post addressing current data regarding polices will be published shortly.
Researchers Kathryn E. Davis, Alexandra E. Edwards, and Diane K. King have looked at data ranging from 1972 to 2016 to assess the efficacy of policies related to alcohol use during pregnancy. View their full article here.
The authors specifically looked at how both supportive policies and punitive policies impacted alcohol use during pregnancy. A supportive policy is any policy that addresses an issue by assisting or educating those affected, while a punitive policy is any policy that addresses an issue using punishment.
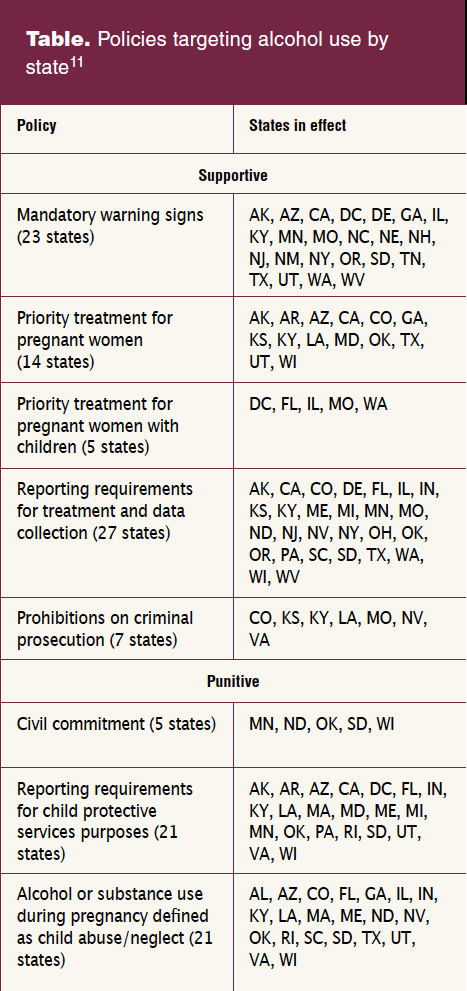
Addressing this complex issue is not easy, but 43 states have laws regarding alcohol during pregnancy. These policies are either punitive or supportive. Fourteen states employ only supportive policies, such as mandatory warning signs, priority substance misuse treatment for pregnant persons with children and pregnant persons without children, prohibitions on criminal prosecutions, and reporting requirements for data and treatment purposes. Four states use only punitive policies, like civil commitment, reporting requirements for use by Child Protective Services, and categorizing alcohol or substance use during pregnancy as child abuse or neglect. Twenty-five states use a mix of both punitive and supportive policies. See full list here
Perhaps surprisingly, data collected between 1985 and 2016 shows that pregnant adults in states without policies regarding alcohol use during pregnancy had a lower likelihood of alcohol use during pregnancy compared to those in states with such policies. Another study looking at data from 1972 to 2013 has further shown this trend. The study revealed that mandatory warning signs, requirements for reporting for child abuse and neglect purposes, priority treatment for pregnant persons, civil commitment policies, and defining alcohol use during pregnancy as child abuse/neglect were associated with increased likelihoods of adverse birth outcomes. These adverse birth outcomes were low birth weight, premature births, and increased need for late prenatal care.
Why is it that state policies addressing alcohol use during pregnancy do not seem to be effective in curbing the practice? Firstly, punitive polices perpetuate negative stereotypes and increase stigma. Supportive polices can also contribute to negative stereotypes, and their impacts can vary between racial groups. These policies can attribute blame and place responsibility solely on those able to be pregnant.
Secondly, the focus should be on implementing policies that allow the health care system to use practices promoting alcohol-free pregnancies. One such practice is alcohol screening and brief intervention (ASBI), a routine preventive practice effective at reducing alcohol misuse for adults without an alcohol use disorder. This practice is non-stigmatizing and requires only positive reinforcement of low-risk behaviors. Policies making it easier for healthcare organizations to practice ASBI could lead to improved outcomes and lower rates of alcohol use during pregnancy.
This analysis highlights the need for more research to identify policies that will reduce alcohol consumption during pregnancy. It also highlights the fact that alcohol use during pregnancy, and FASD in general, is not just an issue for pregnant persons or those with FASDs; all systems of care must be FASD informed and responsibility for increasing positive outcomes must be shared. We can also infer that support for those affected by FASD, not just preventive measures, is critical.

{kind=link}